Minimum DataBase
Multiple myeloma case study: Sydney
Courtesy of Brigitte Wilkens DrMedVet, DipECVIM-CA, MRCVS, Internal Medicine Consultant IDEXX

Background information
Name: Sydney
Age: 14 years
Breed: Labrador Retriever cross
Gender: Female spayed
Presenting reason
Hind limb ataxia and paralysis of the tail
History
Hind limb ataxia and the inability to raise the tail for one week. Weight loss and reduced appetite noticed during last month.
Physical examination
Sydney was bright, alert and responsive. The BCS was low (2/9).
She showed a mild ataxia of both hind legs. There was a complete loss of tail tonus, but normal anal tone. Palpation of the caudal lumbar vertebrae was painful. Proprioception was mildly delayed in both hind limbs and normal in front limbs. Spinal reflexes were normal in all four legs.
Diagnostic plan
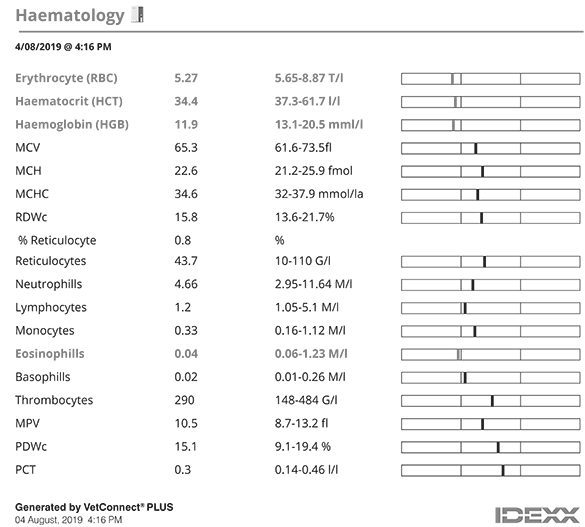
Complete blood count, chemistry profile, electrolytes and urinalysis was performed as minimum database (MDB) given her age and vague clinical signs like weight loss and reduced appetite. Due to hind limb ataxia and the neurologic localization of the lesion, conscious x-rays of the lumbar vertebrae and os sacrum in lateral view were performed.
Interpretation of results
The CBC was unremarkable apart from a mild non-regenerative anaemia, which was thought to be a nonspecific finding and secondary to the underlying problem.
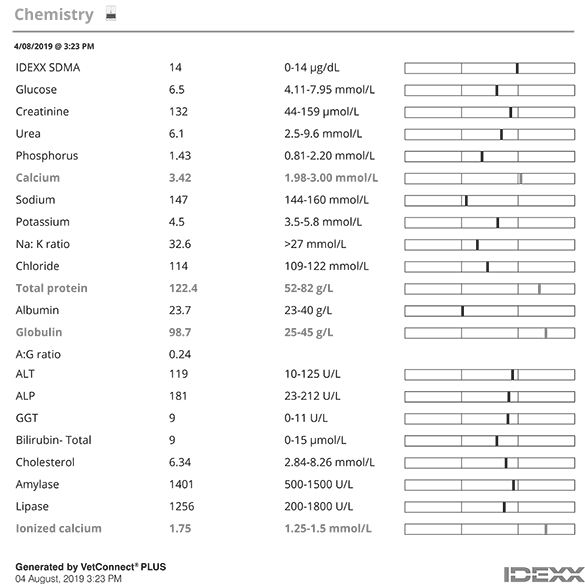
The chemistry profile revealed a marked hyperglobulinemia and hypercalcaemia based on total calcium. Hypercalcaemia was confirmed by measurement of ionized calcium.
Hyperglobulinaemia could be monoclonal or polyclonal. Monoclonal hyperglobulinaemia could be caused by multiple myeloma, lymphoma, lymphatic leukaemia, or less commonly by infectious disease (e.g. leishmaniasis, ehrlichiosis).
Polyclonal hyperglobulinaemia could be the result of chronic inflammatory and infectious diseases, neoplasia, or immune-mediated diseases.
Hypercalcaemia could have been malignancy-associated (e.g. lymphoma, multiple myeloma, apocrine gland carcinoma of anal sac, primary or metastatic bone neoplasia), due to hypoadrenocorticism, primary hyperparathyroidism, granulomatous diseases, hypervitaminosis D, and renal failure.
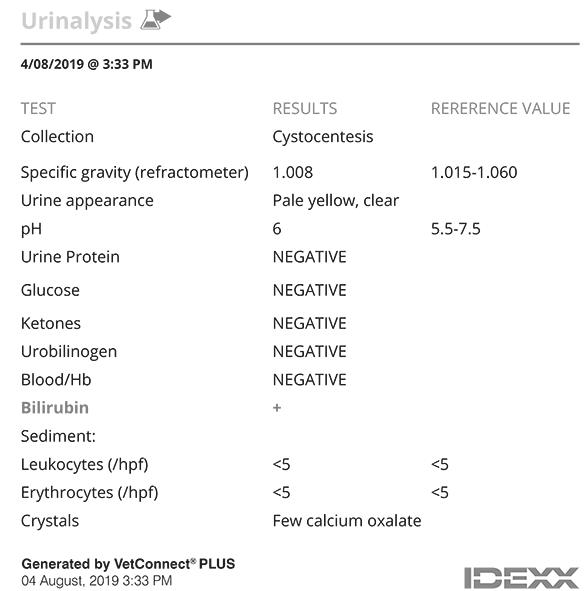
Urine specific gravity was 1.008 and sediment was inactive. The low urine specific gravity was thought to be secondary to hypercalcaemia.
X-rays of the caudal vertebrae were unremarkable.
Due to finding of both, hyperglobuinaemia and hypercalcaemia in the presented case, multiple myeloma or lymphoma was considered most likely. Proprioceptive ataxia could be related (e.g. spinal involvement), however, concurrent disease (e.g. disc protrusion) unrelated to the clinicopathologic findings cannot be ruled out.
Further work-up/next steps:
Serum protein electrophoresis was performed to evaluate the nature of hyperglobulinaemia, urine protein electrophoresis to identify Bence-Jones proteinuria. Hyperglobulinaemia was identified as monoclonal with a narrow spike in the gamma region. Monoclonal hyperglobulinaemia supported the assumption of a neoplastic disease and made an infectious disease less likely. On urine protein electrophoresis revealed no evidence of Bence-Jones proteins.
Under general anaesthesia, abdominal ultrasound, bone marrow aspiration and radiographs of thorax and long bones were carried out.
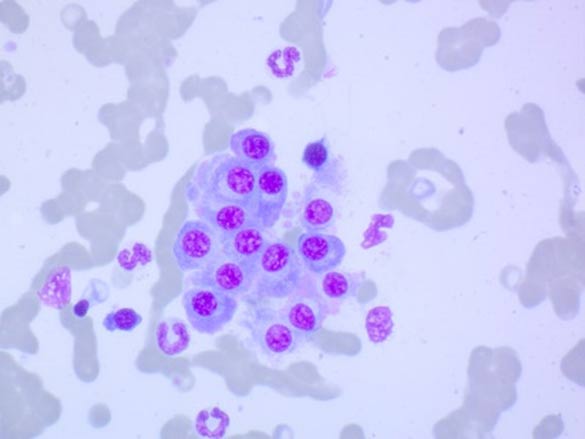
Abdominal ultrasound revealed an enlarged spleen with multiple hypoechoic nodules. Fine needle aspiration of the spleen was performed. Cytology of the spleen showed predominantly round cells with light blue cytoplasma, perinuclear clearing, round nuclei and clumped chromatin. A diagnosis of a plasma cell tumour was made.
Plasma cell infiltration was also observed on bone marrow smears. Multiple plasma cells were seen, characterized by pale blue cytoplasm and largely round basophilic nuclei. In addition, some polynuclear giant cells were present.
On radiographic examination, osteolytic lesions were detected in sternum and multiple long bones.
Diagnostic tests
Additional test results
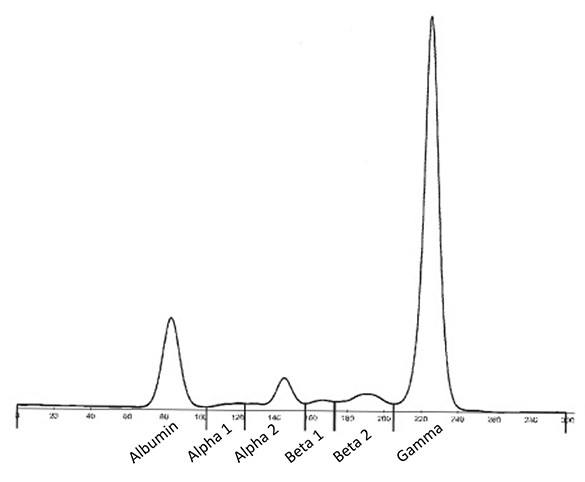
Serum protein electrophoresis: Narrow spike-like peak in gamma region indicating monoclonal hyperglobulineamia
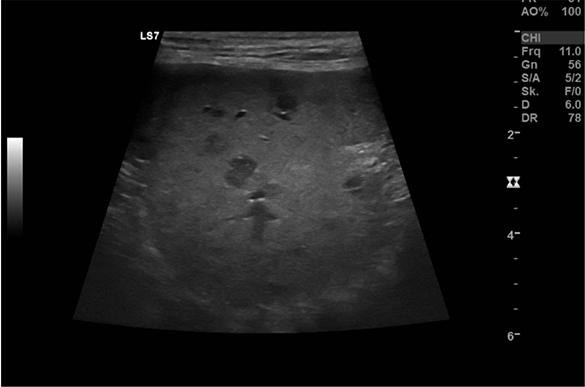
Ultrasound image of the spleen showing hypoechoic nodules

Radiograph of right humerus: extensive bony lysis
Radiograph of right humerus: extensive bony lysis
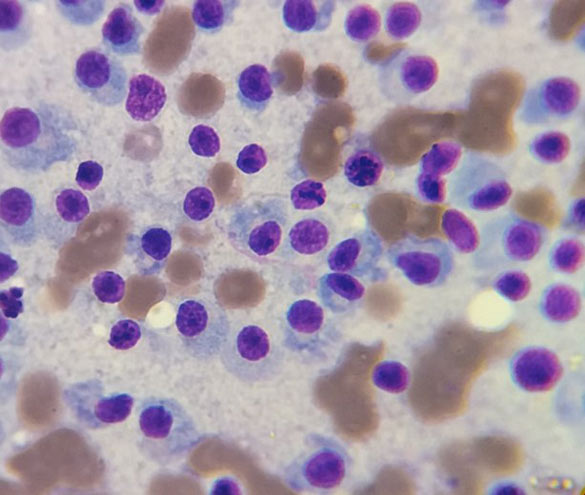
Cytology of bone marrow smear
Diagnosis
Sydney was diagnosed with multiple myeloma based on the presence of hyperglobulinaemia, osteolytic lesions in multiple bones and a plasma cell infiltration into spleen and bone marrow.
Treatment
Sydney was admitted to the hospital for fluid diuresis with 0.9% sodium chloride to treat hypercalcemia. She was also started on buprenorphine for pain relief, which was switched to tramadol and gabapentin on discharge from hospital.
Following diagnosis of multiple myeloma, Sydney was started on melphalan, an oral alkylating agent, in combination with prednisolone. Melphalan was prescribed at 0.1mg/kg/d for the first 10 days. To avoid splitting of tablets (tablet size 2mg) and to achieve the correct cumulative dosage, the patient weighing 23 kg was given 1 tablet each day plus an additional tablet on day 1. Prednisolone was initiated at 0.5 mg/kg/d. Starting on day 11, melphalan dose was continued on 0.05 mg/kg/d long-term, hence, one tablet was administered each day for 4 days per week with no tablet given on the other 3 days. Simultaneously, Prednisolone was reduced to 0.5 mg/kg every other day and stopped after 2 months.
Follow up
Sydney was discharge from hospital once calcium was back to normal. She was seen for regularly re-checks to assess treatment response and to monitor for side effects of melphalan.
She improved progressively and made a full clinical recovery. Ataxia and tail paralysis disappeared completely during first two months of treatment. Globulin values decreased to 48 g/l, but normal values were never reached.
Treatment with melphalan and prednisolone was very well tolerated. Since the most common side effect of melphalan is myelosuppression, a CBC was performed every two weeks for the first two months of treatment and once monthly thereafter. Anaemia resolved and CBCs did never show any significant cytopenia.
Discussion
Multiple myeloma is a systemic proliferation of malignant plasma cells or their precursors typically originating from the bone marrow. Neoplastic cells can metastasize widely, having a predilection for bone and resulting in osteolysis. The malignant transformation of a single plasma cell can secrete a homogenous immunoglobulin product, which often appears as a sharp, well-defined peak or monoclonal gammopathy on serum electrophoresis.
Sydney was presented because of hind limb ataxia and tail paralysis, which suggests a neuroanatomic localisation in the L3-S3 segment. X-rays of the neuroanatomic location did not reveal any abnormalities. Only by performing the MDB, hypercalcaemia and hyperglobulinaemia were detected. Subsequent further work-up lead to the discovery of a well treatable condition. Indeed, multiple myeloma mostly is a rewarding disease to treat since chemotherapy can greatly extend quality and duration of life. The overall response rate for dogs treated with melphalan and prednisone is 92%, with 43.2% of dogs achieving a complete response, the median survival time 540 days. However, cure cannot be expected and eventual relapse during therapy is likely.
Diagnosing multiple myeloma in dogs requires demonstration of at least two of the following criteria: bone marrow plasmacytosis, presence of osteolytic bone lesions, monoclonal hyperglobulinaemia, and Bence-Jones proteinuria. In the present case the diagnosis was based on a monoclonal hyperglobulinaemia, osteolytic lesions in several bones, and eventually plasma cell neoplasia in bone marrow. Detection of plasma cell infiltration into the spleen once more confirmed the disease. Urine protein electrophoresis did not show evidence of Bence-Jones proteinuria; however, its finding was not essential for diagnosis of multiple myeloma, and indeed, in only 25-40% of dogs Bence-Jones proteins are detected in urine.
Although Sydney had hypercalcaemia and extensive bony lysis, both suggested as negative prognostic factors, she made a good clinical recovery. Sydney’s quality of life did improve markedly on treatment, and, by the time this case report was written, she was in partial remission for over a year.
References:
- Seth M, Drobatz KJ, Church DB, et al. White blood cell count and the sodium potassium ratio to screen for hypoadrenocorticism in dogs. J Vet Intern Med 2011; 25:1351-1356
- Sutherland-Smith J, Penninck DG, Keating JH, et al. Ultrasonographic intestinal hyperechoic mucosal striations in dogs are associated with lacteal dilation. Vet Radiol Ultrasound 2007; 48:51-57.
- Shales CJ, Warren J, Anderson DM, et al. Complications following full-thickness small intestinal biopsy in 66 dogs: a retrospective study. J Small Anim Pract 2005; 46:317- 321.
- Zoran D. Protein-losing Enteropathies. In: Bonagura JD, Twedt DC, eds. Kirk’s Current Veterinary Therapy XV. St. Louis: Saunders Elsevier; 2014: 540-544.